Wan Wu1,
Wei Chen2,
Qiong Jin2 ![]()
For correspondence:- Qiong Jin Email: asdjinqiong@hotmail.com Tel:+8657788855488
Received: 1 July 2015 Accepted: 5 February 2016 Published: 31 March 2016
Citation: Wu W, Chen W, Jin Q. Oral mucoadhesive buccal film of ciprofloxacin for periodontitis: preparation and characterization. Trop J Pharm Res 2016; 15(3):447-451 doi: 10.4314/tjpr.v15i3.3
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To prepare and characterise ciprofloxacin mucoadhesive buccal films for localised, improved drug delivery in periodontitis.
Methods: Ciprofloxacin-loaded buccal films containing 50 mg ciprofloxacin were prepared mucoadhesive polymers sodium cellulose (SCMC) and sodium alginate, using a solvent evaporation method. The films were evaluated in terms of thickness, weight, folding endurance, surface pH, drug content, swelling, mucoadhesive properties, release characteristics, and in vivo anti-periodontitis activity, using ampicillin as the standard.
Results: The buccal films showed good drug loading (94.50 ± 0.04 to 99.69 ± 0.21 %) and significant mucoadhesion in terms of in vitro residence time, as well as significant swelling (38.20 ± 1.62 to 54.42 ± 2.32 %). In addition to the good physicochemical properties of the films, ex vivo drug release was high (83.22 ± 1.42 to 90.24 ± 2.01 after 12 h. The films displayed potent anti-periodontitis activity, as indicated by a significant reduction in the bacterial count in a periodontitis model. The samples treated with BFC4 formulation (containing 3:1 SCMC and sodium alginate) exhibited the lowest growth of colonies (57 ± 2.02 CFU/mL) compared with those treated with the BFC3 formulation (69 ± 2.41 CFU/mL) and the standard (80 ± 5.22 CFU/mL).
Conclusion: Formulation BFC4 has suitable physicochemical, drug-release, and anti-periodontitis activity for buccal administration
Introduction
Drug delivery via an oral route is preferred for the treatment of a variety of local and systemic diseases. Periodontitis is an inflammatory disease of the gums that damages the soft tissues and bones that support the teeth. Periodontitis is caused by pathogens such as Porphyromonas gingivalis, Prevotella intermedia, and Aggregatibacter (Actinobacillus) actinomyce-temcomitans. The treatment of periodontitis includes the suppression and elimination of subgingival periodontal pathogens, which require sustained delivery of antibacterial agents [1-4].
Oral controlled delivery can be achieved using a number of drug delivery systems, including strips, gels, films, and implants [5-9]. Additional synergistic effects can be achieved the strategy of mucoadhesion, which prolongs the residence time of the dosage form at the site of absorption and facilitates intimate contact between the dosage form and underlying absorption surface to improve and enhance the bioavailability of drugs.
Ciprofloxacin hydrochloride is a second-generation fluoroquinolone is an antibiotic that is against a wide range of Gram-negative and G-positive facultative bacteria, including periodontal pathogens. It has a biological half-life of 3~4 h, thus requiring frequent dosing [10-12].
Mucoadhesive buccal films can be used to overcome this problem [6,8,13]. Therefore, ciprofloxacin mucoadhesive buccal films were formulated using sodium carboxymethyl cellulose (SCMC) and sodium alginate polymers. In microspheres, these mucoadhesive polymers prolong the residence time of the dosage form in the gastrointestinal tract and are more suitable as matrix material for oral controlled release.
The films were evaluated in terms of their thickness, weight, folding endurance, surface pH, drug content, swelling, mucoadhesive properties, release characteristics and in vivo anti-periodontitis activity.
Methods
Materials
Ciprofloxacin hydrochloride, sodium carboxymethyl cellulose high-viscosity grade, and sodium alginate were purchased from Sigma Aldrich, USA. All other reagents used were of analytical grade.
Preparation of mucoadhesive buccal film of ciprofloxacin
The ciprofloxacin prepared using a solvent-casting method [13,14]. SCMC and sodium alginate were used as mucoadhesive polymers. A certain amount of polymer was dissolved in 20 mL distilled water, and 250 mg ciprofloxacin hydrochloride was added to this solution with continuous stirring, until a homogeneous solution formed. The desired quantity (2 % w/v) of glycerol was added to the homogenised drug polymer solution as a plasticiser. Then, the polymer solution was transferred to a previously prepared glass block and kept at room temperature for drying. The dried film was cut to the desired size, wrapped in aluminium foil, and kept in a desiccator until used.
Evaluation of the physicochemical properties
For prepared films, we evaluated the weight (a 2 × 2 cm piece using a digital balance), thickness (using a micrometre screw gauge), surface pH (after 4 h on an agar plate in an incubator maintained at 37 ± 0.2 °C), swelling percentage (expressed in terms of the increase in film weight after 2 h on an agar plate at 37 ± 0.2 °C), folding endurance (number of times a small strip of film could be folded at the same place before breaking), and drug content (a film was dissolved in 100 mL methanol, stirred for 4 h, and then quantified at 272 nm in a ultraviolet (UV) spectrophotometer) (n=3) [13,14].
Determination of the in vitro residence time
The in vitro residence time was determined using an USP disintegration apparatus, as reported. This method records the time required for complete erosion or dislodgement of the film from the mucosal surface (segments of porcine buccal mucosa glued on a glass slab and placed in a moving disintegration apparatus in phosphate buffer (PB) at pH 6.6 and 37 ± 2 °C) (n=3).
Ex vivo permeation studies
Ex vivo permeation studies of ciprofloxacin mucoadhesive buccal films were conducted in a modified Franz diffusion cell using an excised layer of porcine buccal mucosa. The medium (15 mL PB at pH 7.4) in the receptor compartment was stirred with a magnetic stirrer (at 400 rpm) maintaining a temperature of 37 ± 1 °C. Samples were withdrawn at different times up to 12 h and analysed spectrophotometrically.
Assessment of in vivo anti-periodontitis activity
Adult Wistar rats with a mean weight of 180–200 g were acclimatised for 1 week before the experiment. Five rats were housed per group at a temperature of 23 ± 1 °C and relative humidity of 60 ± 5 % with free access to water and food.
General anaesthesia was obtained by intramuscular injection of a solution of ketamine 10 % and xylazine 2 % (2:1) at 0.12 mL/100 g body weight. The animals were kept on an operating table, with their mouths opened to access the teeth. Ligatures of non-absorbable sterile silk thread were tied around the lower incisors in a figure “8”. The ligature was left in place for 14 days as a gingival irritant and resulted in the development of plaque and periodontitis. The animals were kept in a uniform environment for 14 days and were checked daily to evaluate the suture, food and water intake, and body weight [15,16].
The test group with induced periodontitis was treated with buccal films of ciprofloxacin (BFC4 and BFC3 formulations), the standard group was treated with ampicillin (1.0 mg/disc), and the control group was treated with blank film. The agar well-diffusion method was used to determine the anti-periodontitis activity. The gingiva was swabbed with sterile cotton swabs, which were then swabbed on nutrient agar and potato dextrose agar plates, and the microbial growth was determined after 2 days.
Statistical analysis
The results are expressed as means ± standard deviation. The statistical analysis was performed using Origin 9 (USA). The groups were compared using one-way analysis of variance. P < 0.05 was considered statistically significant.
Results
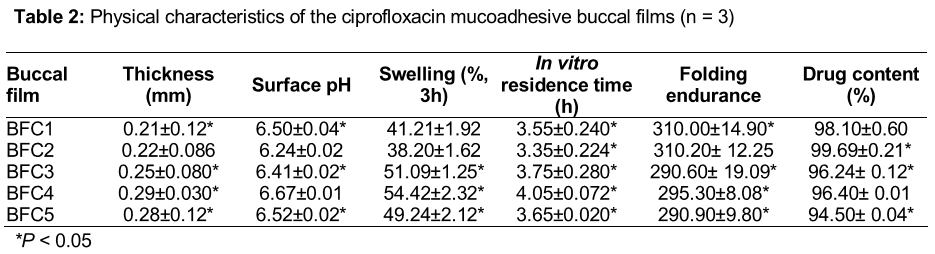
Mucoadhesive buccal films of ciprofloxacin hydrochloride were prepared using SCMC and gelatin by a solvent casting method. Buccal films containing different proportions of the polymers were generated (). The physicochemical properties of the films were evaluated, including the thickness, weight, folding endurance, surface pH, drug content, swelling percentage, in vitro residence time, and mucoadhesive properties ().
The film thicknesses ranged from 0.21 ± 0.12 to 0.29 ± 0.030 mm, the weight ranged from 120 ± 2.04 to 170 ± 2.02 mg, and the surface pH ranged from 6.24 ± 0.02 to 6.67 ± 0.01. All of the films had good folding endurance, and none showed any cracks below 290. The films showed good swelling in the swelling study. The swelling percentage of the films ranged from 38.20 ± 1.62 to 54.42 ± 2.32 % in the following order of formulations: BFC4 > BFC3 > BFC5 > BFC1 > BFC2. The in vitro residence time ranged from 3.35 ± 0.224 to 4.05 ± 0.072 h. The drug content was very good for all formulations (94.50 ± 0.04 to 99.69 ± 0.21%).
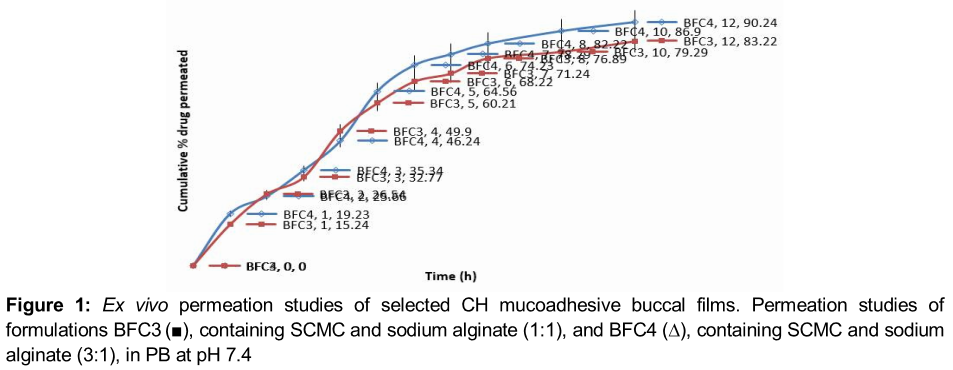
An ex vivo permeation study was performed for formulations BFC3 and BFC4, which had good physicochemical properties (including a high drug content, swelling percentage, and in vitro residence time). The drug release was significantly higher for BFC4 (90.24 ± 2.01 %) than for BFC3 (83.22 ± 1.42 %) at the end of the 12 h ex vivo permeation study ().
The CFU/mL was reduced significantly for the samples cultured with the test groups compared with the control and standard (). The BFC4-treated samples had the lowest CFU (57 ± 2.02 CFU/mL) compared with BFC3-treated samples (69 ± 2.41 CFU/mL) and the standard (80 ± 5.22 CFU/mL).
Discussion
An acidic or alkaline pH may irritate the buccal mucosa and affect the degree of polymer hydration. Therefore, the surface pH of the buccal films was selected to optimise both drug permeation and mucoadhesion [13,14]. Attempts were made to keep the surface pH as close to buccal/salivary pH as possible. The surface pH of all films was the salivary pH.
The effect of swelling behaviour on the residence time of ciprofloxacin hydrochloride on films prepared from various mucoadhesive polymers was also observed The comparative swelling of various formulations was in the order BFC4 > BFC3 > BFC5 > BFC1 > BFC2. Swelling has been reported to have a significant effect on the residence time of buccal films [13,14]. In a recent study, the swelling of HEC films was reduced by the addition of Carbopol 934P and Eudragit-RL100, but was increased by the addition of SCMC in verapamil hydrochloride buccal films [17]. In general, the films with the highest degree of swelling had greater residence times, while the films with the least swelling had shorter residence times. Formulation BFC3 (prepared with sodium alginate) had the least swelling and the shortest residence time.
The ex vivo permeation was also reported to be good for SCMC-like polymers. Semalty et al reported greater drug permeation with SCMC-containing buccal film [13]. Note that the water solubility profiles of the drug evaluated in that study (diltiazem HCl) and ciprofloxacin HCl are similar. Thus, their results support the percentage of drug permeation.
The ex vivo release characteristics and in vivo anti periodontitis activity indicated that BFC3 and BFC4 were very effective for treating periodontitis. BFC4 showed better release and better anti-periodontitis activity. The anti-periodontitis activity of both films was better than that of the standard (ampicillin).
Studies have reported the anti-periodontitis activity of films or other localised oral mucosal or gingival drug delivery systems [18-23]. Many studies have reported on the potential of novel ciprofloxacin delivery devices in the treatment of periodontitis [24-27]. Among these studies, films showed promising results.
Conclusion
Mucoadhesive buccal films of ciprofloxacin hydrochloride prepared using mucoadhesive polymers had satisfactory physicochemical properties, good drug-loading and mucoadhesive properties, and high ex vivo permeation and anti-periodontitis activity. Buccal film formulation BFC4 (containing SCMC and sodium alginate in a 3:1 ratio) had the best physicochemical, drug-release, and anti-periodontitis activity.
References
Archives


News Updates